

PELVIC ORGAN PROLAPSE AND SPINA BIFIDA
Jake Miller, Benjamin Yu, and Stephanie Kielb MD
Women with spina bifida have multiple risk factors for experiencing pelvic organ prolapse.
Co-existing conditions often predispose women to additional risk of experiencing pelvic organ prolapse. FEW women are aware that POP is a condition to be concerned about until after they are diagnosed, including those with comorbid conditions. With a nod to Spina Bifida Association, here is some basic info to shine a light.
1. What is spina bifida?
Spina Bifida (SB) is a birth defect in which the bones that protect the spinal cord, or vertebrae, do not completely cover the spinal cord.
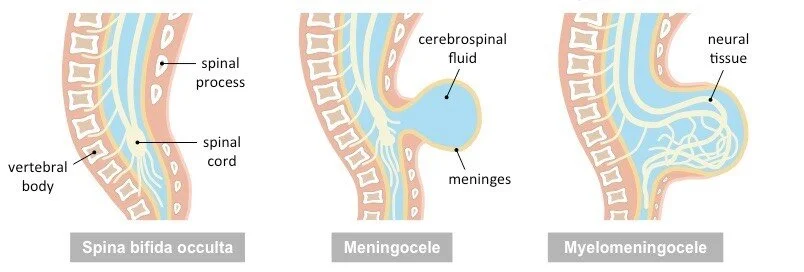
Spina bifida can range widely in severity. The mildest form, called “spina bifida occulta”, occurs when there is only a small gap in these vertebrae - the bones of the spine. This is the most common type of SB and rarely causes symptoms. More severe is when the tissue that covers the spinal cord protrudes through this gap in these bones, called a “meningocele”. The most severe form is when both the spinal cord and its covering protrude through this gap, a condition called “myelomeningocele”. Patients with “myelomeningocele” oftentimes experience issues with the nerves of the lower body, which can result in paralysis, loss of sensation, or difficulties with bowel and bladder function (1).
2. How common is pelvic organ prolapse (POP) in women with SB?
Though this has not been thoroughly studied, it has been reported that about 1 in 2 women with SB will develop pelvic organ prolapse (POP), a protrusion of the pelvic organs (i.e., the uterus, intestines or bladder) through the vagina (2). This is similar to the risk for women in the general population (3,4).
However, women with SB may develop POP with fewer risk factors compared to women who are otherwise healthy. For example, while vaginal birth is a well-established risk factor for POP, many women with SB who have never given birth still frequently develop POP (2,5,6). There are many other congenital conditions, including Ehler’s Danlos, bladder exstrophy, and cloacal exstrophy, that also place women at higher risk of POP independent of vaginal birth.
3. At what age does POP tend to manifest?
Women with SB develop POP at an average age of 33 years old (2). This is quite similar to women in the general population, where most women present between ages 25-45 (4). It is important to keep in mind, however, that POP can develop at any time between a woman’s teenage years up through the end of life.
4. How does SB impact strength and integrity of pelvic floor muscles and why?
There are many ways SB can directly and indirectly impact the integrity of the pelvic floor muscles, which are the muscles that hold up the pelvic organs. Directly, many patients with SB are affected at their mid and lower spines, where the nerves that control the pelvic floor muscles are found. SB can damage these nerves, resulting in the weakening of the pelvic floor and POP (7). The pelvic muscles and pelvic floor may also develop differently in those with SB, which may cause those with SB to have weaker pelvic floors at baseline. This weakness places those with SB at a higher risk of POP, regardless of any nerve involvement.
Indirectly, SB may worsen some of the general risk factors, and thus the likelihood, of developing POP. One of the main risk factors for POP is high abdominal pressure. This can occur due to several causes, including straining from constipation, repetitive lifting, and transferring from seated to standing positions (8). Those with SB, for example, are at a high risk of long-term constipation due to nerve damage, which increases their risk of developing POP (9,10). Additionally, many women with SB experience reduced or absent pelvic sensation and may not notice the common symptoms of POP as they develop (2). As such, patients with SB and POP may wait longer periods of time before seeking treatment, during which their POP may worsen.
5. Are routine pelvic exams standard practice in women with SB?
Yes, patients with SB should receive routine pelvic exams. Since women with SB tend to have reduced or absent pelvic sensation, they may not experience the typical symptoms of POP that would prompt them to seek medical care. As a result, routine pelvic examinations are important for the early detection and treatment of POP. Patients with SB may also face difficulties regarding sexual function and pregnancy, and oftentimes find it difficult to connect with their physicians in regard to these concerns (11). Routine exams can promote early and regular discussions with one’s medical provider on health issues that might otherwise be overlooked.
6. Which POP symptoms to SB patients experience?
POP symptoms vary greatly between women and depend on many factors, including the severity of one’s POP and a woman’s level of sensation at baseline. While women with milder POP may not experience any bothersome symptoms, those with more advanced POP can experience vaginal pressure, tissues bulging from the vagina, and pain during intercourse (2).
7. What w/b the most beneficial path for POP treatment in SB, nonsurgical or surgical treatment (do nonsurgicals have any value if pc muscle strength can’t be improved)?
The right treatment for POP varies greatly between women and depends on one's symptoms, overall health, and personal preferences. Because of the complexity that goes into choosing the appropriate treatment, it is recommended that all women with SB and POP seek out appropriate help before choosing a treatment plan. Depending on the extent to which SB has affected a woman’s lifestyle and body, it may be necessary to tailor common treatments to better fit a specific person’s case. Thus, it is recommended that those with SB and POP seek out a Urologist specializing in female pelvic medicine and reconstructive surgery, as they would be most experienced at managing patients with neurogenic bladder. Since SB patients are also at greater risk for kidney stones, urinary tract infections, problems with kidney function, and some types of cancer, these women typically need life-long urologic care. In fact, many of these women have required complex surgeries to reconstruct their urinary tract (10). As such, it is important for women with SB to seek out care from a urologist with experience caring for SB patients (12,13).
With regard to specific treatments, when POP is not severe or when symptoms are not bothersome, it may be appropriate to forego any interventions and instead, closely monitor a patient's POP over time for changes.
For those who are seeking treatment, but are unable to undergo surgery or prefer to first try nonsurgical treatments, vaginal pessaries are a common option (2). These devices are inserted into the vagina to hold the pelvic organs in place (12). Many women with mild POP also choose to try pelvic floor physical therapy as a form of treatment. However, it is unknown if physical therapy is as helpful for women with SB as they commonly have underlying issues with their pelvic floor, muscles, and nerves.
There are many different surgical options for POP as well. Common procedures include: 1. Uterosacral Ligament Suspension or Sacrospinous Ligament Suspension – procedures, commonly performed at the same time as a hysterectomy, or removal of the uterus, in which the pelvic organs are supported using the surrounding body walls or spine, 2. Sacrocolpopexy - a procedure in which the pelvic organs are supported using connections to the lower spine, and 3. Colpocleisis - a procedure in which the front and back walls of the vagina are closed to prevent future bulging (14). These surgeries differ in their effectiveness as well as their impact on quality of life and sexual functioning. Thus, it is highly recommended that women with SB who are seeking surgical treatment for their POP first discuss their symptoms and goals with a specialized Urologist to see which option is most appropriate for them.
Jake Miller, Benjamin Yu, and Stephanie Kielb MD
Northwestern University
Feinberg School of Medicine
Chicago, IL
Bibliography
1. "What is Spina Bifida?" Spina Bifida Association, Spina Bifida Association, 6 Apr. 2020, www.spinabifidaassociation.org/what-is-spina-bifida-2/.
2. Liu JS, Vo AX, Doolittle J, Hamoui N, Lewicky-Gaupp C, Kielb SJ. Characterizing pelvic organ prolapse in adult spina bifida patients. Urology. 2016 Jun 24;97:273–276.
3. Barber MD, Maher C. Epidemiology and outcome assessment of pelvic organ prolapse. Int Urogynecol J. 2013 Nov;24(11):1783–1790.
4. Swift S, Woodman P, O’Boyle A, Kahn M, Valley M, Bland D, et al. Pelvic Organ Support Study (POSST): the distribution, clinical definition, and epidemiologic condition of pelvic organ support defects. Am J Obstet Gynecol. 2005 Mar;192(3):795–806.
5. Quiroz LH, Muñoz A, Shippey SH, Gutman RE, Handa VL. Vaginal parity and pelvic organ prolapse. J Reprod Med. 2010 Apr;55(3-4):93–98.
6. Jelovsek JE, Maher C, Barber MD. Pelvic organ prolapse. Lancet. 2007 Mar 24;369(9566):1027–1038.
7. Rintoul NE, Sutton LN, Hubbard AM, Cohen B, Melchionni J, Pasquariello PS, et al. A new look at myelomeningoceles: functional level, vertebral level, shunting, and the implications for fetal intervention. Pediatrics. 2002 Mar;109(3):409–413.
8. Iglesia CB, Smithling KR. Pelvic Organ Prolapse. Am Fam Physician. 2017 Aug 1;96(3):179–185.
9. Awad RA. Neurogenic bowel dysfunction in patients with spinal cord injury, myelomeningocele, multiple sclerosis and Parkinson’s disease. World J Gastroenterol. 2011 Dec 14;17(46):5035–5048.
10. Burke R, Liptak GS, Council on Children with Disabilities. Providing a primary care medical home for children and youth with spina bifida. Pediatrics. 2011 Dec;128(6):e1645–57.
11. Streur CS, Schafer CL, Garcia VP, Quint EH, Sandberg DE, Kalpakjian CZ, et al. He told me it would be extremely selfish of me to even consider [having kids]": The importance of reproductive health to women with spina bifida and the lack of support from their providers. Disabil Health J. 2020 Apr;13(2):100815.
12. "Transitional Urology." Northwestern Medicine, Northwestern Memorial HealthCare, www.nm.org/conditions-and-care-areas/urology/transitional-urology.
13. "Congenital Genitourinary Disorders." Feinberg School of Medicine, Northwestern University, www.feinberg.northwestern.edu/sites/urology/specialties/congenital-genitourinary.html.
14. "Pelvic Organ Prolapse." Voices for PFD, American Urogynecologic Society, www.augs.org/assets/2/6/POP.pdf.